
Longitudinal Changes of Quality of Life and Hearing Following Radiosurgery for Vestibular Schwannoma

 , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Rutten, I.; Baumert, B.G.; Seidel, L.; Kotolenko, S.; Collignon, J.; Kaschten, B.; Albert, A.; Martin, D.; Deneufbourg, J.-M.; Demanez, J.-P.; et al. Long-term follow-up reveals low toxicity of radiosurgery for vestibular schwannoma. Radiother. Oncol. 2007, 82, 83–89. [Google Scholar] [CrossRef]
- Windisch, P.Y.; Tonn, J.; Fürweger, C.; Wowra, B.; Kufeld, M.; Schichor, C.; Muacevic, A. Clinical Results After Single-fraction Radiosurgery for 1,002 Vestibular Schwannomas. Cureus 2019, 11, e6390. [Google Scholar] [CrossRef] [Green Version]
- Myrseth, E.; Pedersen, P.-H.; Møller, P.; Lund-Johansen, M. Treatment of vestibular schwannomas. Why, when and how? Acta Neurochir. 2007, 149, 647–660, discussion 660. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.-W.; Tu, H.-T.; Chuang, C.-Y.; Chang, C.-S.; Chou, H.-H.; Lee, M.-T.; Huang, C.-F. Gamma Knife radiosurgery for large vestibular schwannomas greater than 3 cm in diameter. J. Neurosurg. 2018, 128, 1380–1387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goldbrunner, R.; Weller, M.; Regis, J.; Lund-Johansen, M.; Stavrinou, P.; Reuss, D.; Evans, D.G.; Lefranc, F.; Sallabanda, K.; Falini, A.; et al. EANO guideline on the diagnosis and treatment of vestibular schwannoma. Neurosurg. Oncol. 2020, 22, 31–45. [Google Scholar] [CrossRef]
- Miller, L.E.; Brant, J.A.; Chen, J.; Kaufman, A.C.; Ruckenstein, M.J. Hearing and Quality of Life Over Time in Vestibular Schwannoma Patients: Observation Compared to Stereotactic Radiosurgery. Otol. Neurotol. 2019, 40, 1094–1100. [Google Scholar] [CrossRef]
- Berkowitz, O.; Han, Y.-Y.; Talbott, E.O.; Iyer, A.K.; Kano, H.; Kondziolka, D.; Brown, M.A.; Lunsford, L.D. Gamma Knife Radiosurgery for Vestibular Schwannomas and Quality of Life Evaluation. Stereotact. Funct. Neurosurg. 2017, 95, 166–173. [Google Scholar] [CrossRef]
- Soulier, G.; van Leeuwen, B.M.; Putter, H.; Jansen, J.C.; Malessy, M.J.A.; van Benthem, P.P.G.; van der Mey, A.G.L.; Stiggelbout, A.M. Quality of Life in 807 Patients with Vestibular Schwannoma: Comparing Treatment Modalities. Otolaryngol. Head Neck Surg. 2017, 157, 92–98. [Google Scholar] [CrossRef]
- Carlson, M.L.; Tveiten, O.V.; Driscoll, C.L.; Goplen, F.K.; Neff, B.A.; Pollock, B.E.; Tombers, N.M.; Castner, M.L.; Finnkirk, M.K.; Myrseth, E.; et al. Long-term quality of life in patients with vestibular schwannoma: An international multicenter cross-sectional study comparing microsurgery, stereotactic radiosurgery, observation, and nontumor controls. J. Neurosurg. 2015, 122, 833–842. [Google Scholar] [CrossRef] [Green Version]
- Hayhurst, C.; Zadeh, G. Tumor pseudoprogression following radiosurgery for vestibular schwannoma. Neurosurg. Oncol. 2012, 14, 87–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.S.; Grills, I.S.; Bojrab, D.; Pieper, D.; Kartush, J.; Maitz, A.; Martin, A.; Perez, E.; Hahn, Y.; Ye, H.; et al. Longitudinal assessment of quality of life and audiometric test outcomes in vestibular schwannoma patients treated with gamma knife surgery. Otol. Neurotol. 2011, 32, 676–679. [Google Scholar] [CrossRef] [PubMed]
- Blome, C.; Augustin, M. Measuring change in quality of life: Bias in prospective and retrospective evaluation. Value Health 2015, 18, 110–115. [Google Scholar] [CrossRef] [Green Version]
- Sharma, M.S.; Singh, R.; Kale, S.S.; Agrawal, D.; Sharma, B.S.; Mahapatra, A.K. Tumor control and hearing preservation after Gamma Knife radiosurgery for vestibular schwannomas in neurofibromatosis type 2. J. Neurooncol. 2010, 98, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Kida, Y.; Kato, T.; Iizuka, H.; Kuramitsu, S.; Yamamoto, T. Long-term safety and efficacy of stereotactic radiosurgery for vestibular schwannomas: Evaluation of 440 patients more than 10 years after treatment with Gamma Knife surgery. J. Neurosurg. 2013, 118, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Curran, D.; Molenberghs, G.; Fayers, P.M.; Machin, D. Incomplete quality of life data in randomized trials: Missing forms. Stat. Med. 1998, 17, 697–709. [Google Scholar] [CrossRef]
- Ware, J.E., Jr.; Gandek, B.; Kosinski, M.; Aaronson, N.K.; Apolone, G.; Brazier, J.; Bullinger, M.; Kaasa, S.; Leplège, A.; Prieto, L.; et al. The equivalence of SF-36 summary health scores estimated using standard and country-specific algorithms in 10 countries: Results from the IQOLA Project. International Quality of Life Assessment. J. Clin. Epidemiol. 1998, 51, 1167–1170. [Google Scholar] [CrossRef]
- Santa Maria, P.L.; Shi, Y.; Gurgel, R.K.; Corrales, C.E.; Soltys, S.G.; Santa Maria, C.; Murray, K.; Chang, S.D.; Blevins, N.H.; Gibbs, I.C.; et al. Long-Term Hearing Outcomes Following Stereotactic Radiosurgery in Vestibular Schwannoma Patients-A Retrospective Cohort Study. Neurosurgery 2018, 85, 550–559. [Google Scholar] [CrossRef] [PubMed]
- Chae, R.; McDermott, M.; Muacevic, A.; Adler, J.R., Jr.; Sharon, J.D. Vestibular Migraine Following Radiosurgery for Vestibular Schwannoma. Cureus 2020, 12, e8569. [Google Scholar]
- Fleishman, J.A.; Lawrence, W.F. Demographic variation in SF-12 scores: True differences or differential item functioning? Med. Care 2003, 41, III75–III86. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.E.; Brant, J.A.; Naples, J.G.; Bigelow, D.C.; Lee, J.Y.K.; Ruckenstein, M.J. Quality of Life in Vestibular Schwannoma Patients: A Longitudinal Study. Otol. Neurotol. 2020, 41, e256–e261. [Google Scholar] [CrossRef]
- Cheng, S.; Naidoo, Y.; da Cruz, M.; Dexter, M. Quality of life in postoperative vestibular schwannoma patients. Laryngoscope 2009, 119, 2252–2257. [Google Scholar] [CrossRef]
- Di Maio, S.; Akagami, R. Prospective comparison of quality of life before and after observation, radiation, or surgery for vestibular schwannomas. J. Neurosurg. 2009, 111, 855–862. [Google Scholar] [CrossRef]
- Kufeld, M.; Fürweger, C.; Drexler, C.G.; Wowra, B.; Muacevic, A. Implementation of a medical database system for a radiosurgery center. Cureus 2009, 1, e4. [Google Scholar] [CrossRef] [Green Version]
- Adler, J.R., Jr.; Chang, S.D.; Murphy, M.J.; Doty, J.; Geis, P.; Hancock, S.L. The Cyberknife: A frameless robotic system for radiosurgery. Stereotact. Funct. Neurosurg. 1997, 69, 124–128. [Google Scholar] [CrossRef] [PubMed]
- Resnick, B.; Nahm, E.S. Reliability and validity testing of the revised 12-item Short-Form Health Survey in older adults. J. Nurs. Meas. 2001, 9, 151–161. [Google Scholar] [CrossRef] [PubMed]
- Lim, L.L.; Fisher, J.D. Use of the 12-item short-form (SF-12) Health Survey in an Australian heart and stroke population. Qual. Life Res. 1999, 8, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Ware, J., Jr.; Kosinski, M.; Keller, S.D. A 12-Item Short-Form Health Survey: Construction of scales and preliminary tests of reliability and validity. Med. Care 1996, 34, 220–233. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glickman, M.E.; Rao, S.R.; Schultz, M.R. False discovery rate control is a recommended alternative to Bonferroni-type adjustments in health studies. J. Clin. Epidemiol. 2014, 67, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Benjamini, Y.; Krieger, A.M.; Yekutieli, D. Adaptive linear step-up procedures that control the false discovery rate. Biometrika 2006, 93, 491–507. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Feature | No. of Patients Unless Specified Otherwise | Range (Min–Max) |
|---|---|---|
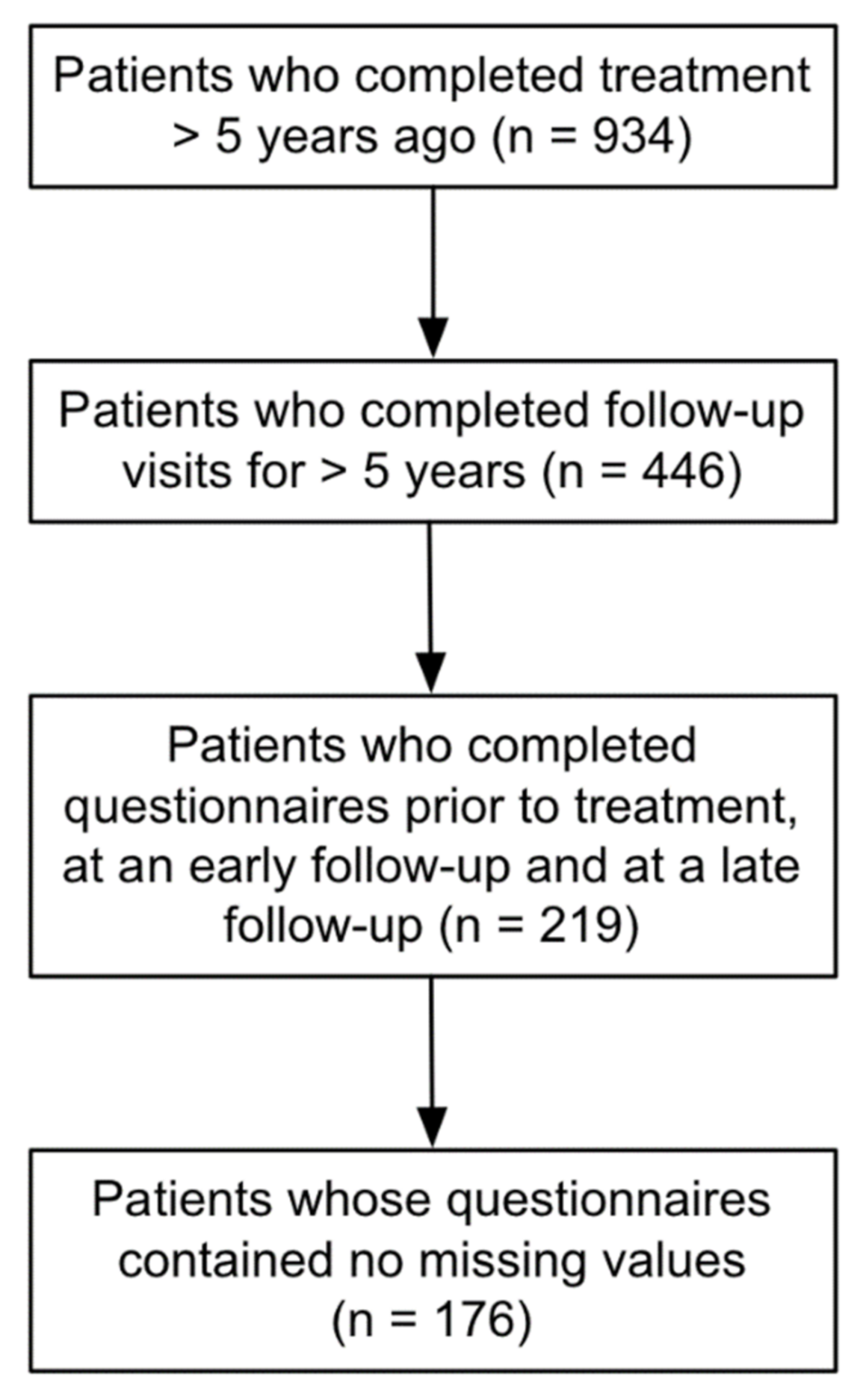
| Number of patients | 176 | |
| Side | ||
| Left | 93 | |
| Right | 83 | |
| Sex | ||
| Male | 78 | |
| Female | 98 | |
| Median age [years] | 55.5 | 15.5–78.5 |
| Prior surgery | 40 (22.7%) | |
| Prior radiotherapy | 5 (2.8%) | |
| NF2-associated tumors | 4 (2.2%) | |
| Median tumor volume [cc] | 0.6 | 0.05–5.9 |
| Median dose [Gy] | 13 | 12–14 |
| Median isodose [%] | 70 | 60–75 |
| Sub-score | Mean Prior to SRS | Standard Deviation | Mean at Early FUP | Standard Deviation | D Early vs. Prior | p (Early vs. Prior) | Mean at Late FUP | Standard Deviation | D Late vs. Prior | p (Late vs. Prior) |
|---|---|---|---|---|---|---|---|---|---|---|
| PF | 85.5 | 23.5 | 80.4 | 26.8 | −5.1 | 0.004 | 80.8 | 28.2 | −4.7 | 0.017 |
| RP | 76.5 | 25.1 | 75.6 | 22.5 | −0.9 | 0.627 | 74.1 | 24.1 | −2.4 | 0.391 |
| BP | 86.2 | 20.7 | 84.5 | 22.8 | −1.7 | 0.325 | 82.5 | 24.6 | −3.7 | 0.054 |
| GH | 61.2 | 20.1 | 62.7 | 20.1 | +1.5 | 0.323 | 63.7 | 21.8 | +2.5 | 0.195 |
| VT | 58.7 | 23.4 | 62.5 | 21.0 | +3.8 | 0.015 | 60.8 | 23.8 | +2.1 | 0.247 |
| SF | 77.1 | 25.3 | 79.1 | 23.8 | +2.0 | 0.314 | 78.0 | 25.9 | +0.9 | 0.715 |
| RE | 75.5 | 25.3 | 77.5 | 23.5 | +2.0 | 0.279 | 77.2 | 24.6 | +1.7 | 0.427 |
| MH | 68.3 | 19.1 | 70.7 | 17.8 | +2.4 | 0.059 | 70.8 | 20.3 | +2.5 | 0.091 |
| PCS | 50.7 | 7.9 | 49.4 | 8.3 | −1.3 | 0.015 | 49.1 | 8.8 | −1.6 | 0.011 |
| MCS | 46.7 | 10.9 | 48.8 | 9.4 | +2.1 | 0.004 | 48.6 | 10.4 | +1.9 | 0.032 |
| Subscore | Mean Prior to SRS | Standard Deviation | Mean at Early FUP | Standard Deviation | D Early vs. Prior | Mean at Late FUP | Standard Deviation | D Late vs. Prior | |
|---|---|---|---|---|---|---|---|---|---|
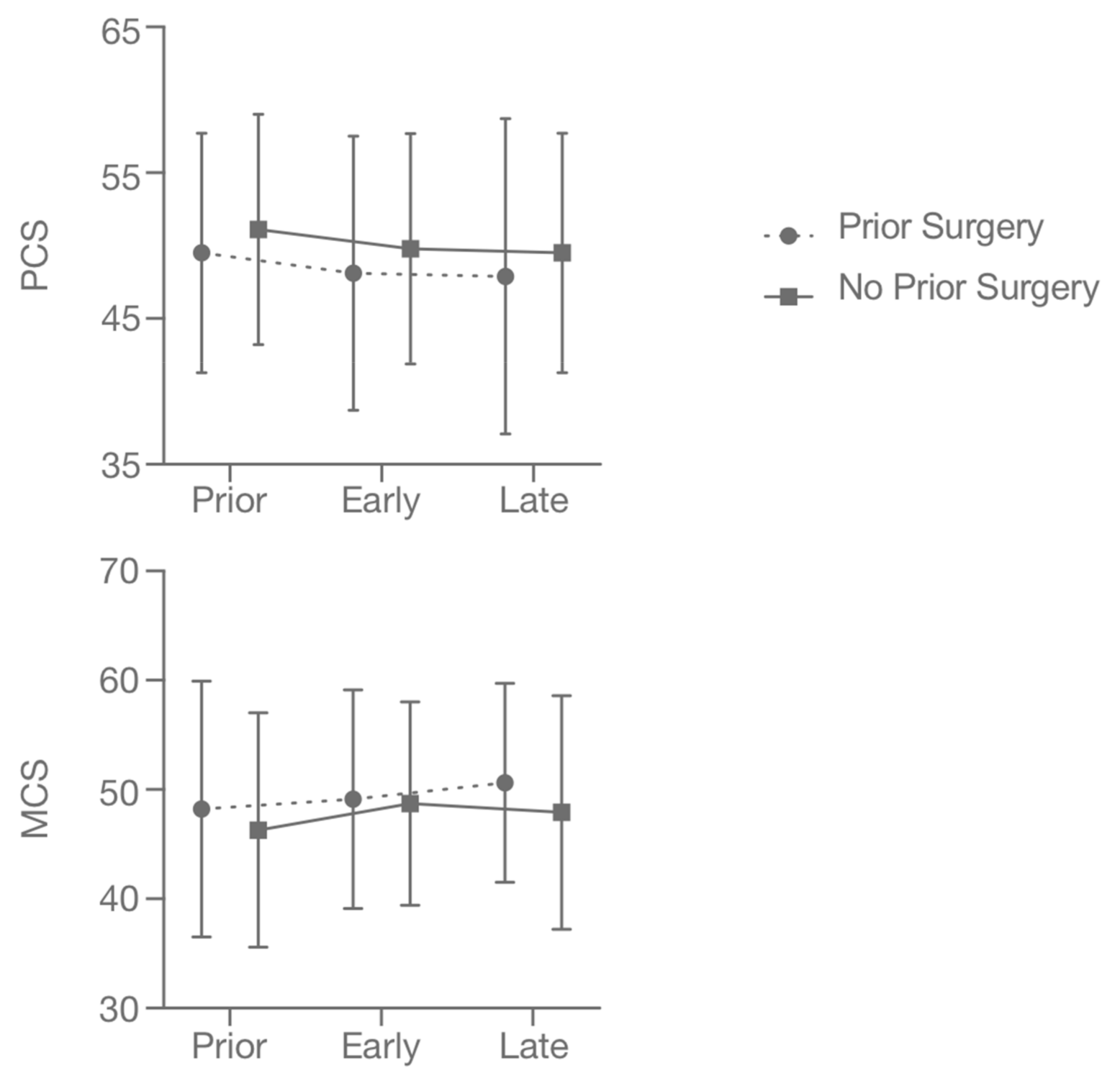
| PCS | Prior surgery (n = 40) | 49.5 | 8.2 | 48.1 | 9.4 | −1.4 | 47.9 | 10.8 | −1.6 |
| No prior surgery (n = 136) | 51.1 | 7.9 | 49.8 | 7.9 | −1.3 | 49.5 | 8.2 | −1.6 | |
| MCS | Prior surgery (n = 40) | 48.2 | 11.7 | 49.1 | 10.0 | +0.9 | 50.6 | 9.1 | +2.4 |
| No prior surgery (n = 136) | 46.3 | 10.7 | 48.7 | 9.3 | +2.4 | 47.9 | 10.7 | +1.6 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Windisch, P.; Tonn, J.-C.; Fürweger, C.; Ehret, F.; Wowra, B.; Kufeld, M.; Schichor, C.; Muacevic, A. Longitudinal Changes of Quality of Life and Hearing Following Radiosurgery for Vestibular Schwannoma. Cancers 2021, 13, 1315. https://doi.org/10.3390/cancers13061315
Windisch P, Tonn J-C, Fürweger C, Ehret F, Wowra B, Kufeld M, Schichor C, Muacevic A. Longitudinal Changes of Quality of Life and Hearing Following Radiosurgery for Vestibular Schwannoma. Cancers. 2021; 13(6):1315. https://doi.org/10.3390/cancers13061315
Chicago/Turabian StyleWindisch, Paul, Jörg-Christian Tonn, Christoph Fürweger, Felix Ehret, Berndt Wowra, Markus Kufeld, Christian Schichor, and Alexander Muacevic. 2021. "Longitudinal Changes of Quality of Life and Hearing Following Radiosurgery for Vestibular Schwannoma" Cancers 13, no. 6: 1315. https://doi.org/10.3390/cancers13061315